Lower Motor Neuron Disorders:
Introduction:
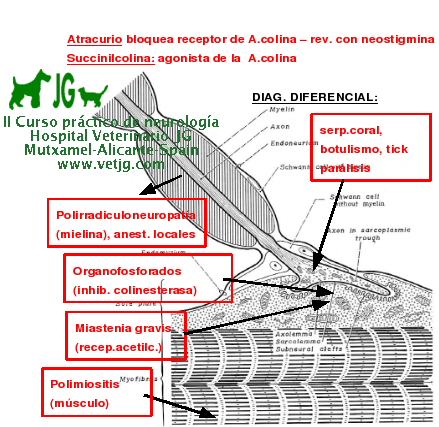
One of the causes of acute quadriparesis or quadriplegia is that of diffuse lower motor
neuronal (LMN) dysfunction, resulting in diminished to absent reflexes in all 4 legs. In this
instance the immediate differential diagnosis must include acute polyradiculoneuropathy, Coral
snake envenomation, tick paralysis, and botulism.
Other causes which normally result in normal
reflexes with progressive weakness on exercise include polymyositis, myasthenia gravis, and
sub-acute organophosphate (OP) intoxication. The nature of these diseases are that they affect
some portion of the lower motor unit.
Polyradiculoneuropathy affects the myelinated fibers of
the motor nerves.
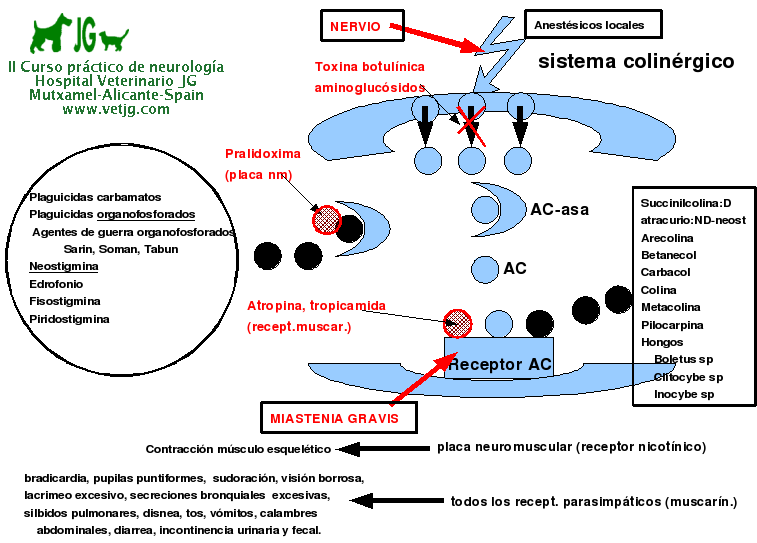
Coral snake envenomation, tick paralysis and botulism result from toxins
which alter the release of acetylcholine at the neuromuscular junction.
Myasthenia gravis and
sub-acute OP intoxication alter the release or responsiveness of the neuromuscular junction to
acetylcholine on repeated neural activity.
Polymyositis directly affects the muscle.
The former
conditions result in flaccid paralysis, while the latter ones result in weakness, stiffness and
collapse on exercise. Coral snakes are limited in their distribution and it should be considered in
cases of LMN disease in areas where they are endemic. The ticks which are associated with tick
paralysis vary and are present throughout the world. Tick paralysis appears to be seasonal, but
can occur at any time. Botulism can occur from food poisoning or from alterations in the
intestinal flora. Dogs are fairly resistant to botulinum toxin, but intoxication is occasionally seen.
Diagnostic Approach:
The diagnosis of motor unit disease requires looking for systemic illness, ruling out
obvious vertebral disease and identifying the specific changes of the disease. This includes many
of the test employed in looking for cervical and TL disease, including CSF tap and analysis. On
the other hand, serum muscle enzyme levels (CPK, AST, LDH and aldolase concentrations)
should be run. In some cases, pre- and post-exercise levels of CPK and lactate can help confirm
the diagnosis. In addition, serum cholinesterase levels are needed to evaluate the potential for OP
intoxication. The most important aspect of the examination are EMG studies, including needle
EMG, nerve conduction velocities and repetitive nerve stimulation. Muscle and/or nerve biopsy
may allow histopathologic diagnosis, muscle immunohistology, fiber typing and enzyme
measurements. In cases of suspected myasthenia gravis, response to edrophonium HCl, a short
acting anticholinergic drug, can be used. Edrophonium given intravenously at 0.1-0.2 mg/kg can
produce dramatic improvements in muscle strength in 1-2 minutes in patients in myasthenic
crisis or who is exercise intolerant. On the other hand, it can worsen the signs of OP intoxication.
For this reason, I prefer to perform edrophonium testing under anesthesia during the EMG
procedure.
POLIRADICULOPATIA
INTOX. POR ORGANOSFOSFORADOS
MIASTENIA GRAVIS
POLIMIOSITIS |